
A client is sitting in your consultation room in Zürich, Lausanne, or Lucerne. She’s read about acids, barrier repair, marine balms, organic oils, and “clean beauty”. She wants brighter skin, less pigment, fewer textural irregularities, and she wants to know one thing before she books.
If a TCA peel is a medical procedure, can it still fit a natural skincare philosophy?
Yes, but only if you understand the peeling process properly. That’s where many clinicians and retail partners get stuck. They know the treatment works, but they don’t always know how to explain tca peel peeling in plain language, how to prepare clients for the day-by-day changes, or how to pair a clinical peel with ethically sourced aftercare without drifting into marketing fluff or unsafe advice.
I teach new clinicians to think of TCA this way. The acid is the intervention. The peeling is the visible phase of repair. The outcome depends on the protocol, the patient selection, and the discipline of aftercare. In Switzerland, climate and regulation make that even more important.
The Rise of TCA Peels in Swiss Aesthetic Practice
In a Swiss consultation room, the conversation often turns on a practical tension. The patient wants more correction than a superficial “glow” treatment can offer, but she does not want a plan that clashes with her preference for cruelty-free formulas, traceable ingredients, and restrained, medically sound care.
This is the context in which TCA has become especially relevant in Swiss practice.
Its appeal is not hard to understand. TCA sits in a useful middle position between light resurfacing and device-based procedures. For clinicians, that means a treatment with visible corrective potential for concerns such as photoageing, uneven tone, and textural change. For patients, it offers a defined treatment path rather than a long cycle of product experimentation.
In Switzerland, that position matters even more because the setting is different. High UV exposure, winter dryness, indoor heating, and frequent travel between mountain and urban environments all place unusual stress on the barrier. At the same time, many Swiss patients read ingredient lists closely and ask whether medical treatments can be paired with cleaner, ethically sourced aftercare. They are not rejecting evidence-based medicine. They are asking whether efficacy and product ethics can sit in the same protocol.
They can, but only with discipline.
A well-run TCA program works like good architectural restoration in an old Swiss town. The intervention is targeted, the endpoint is controlled, and every material used afterward has to support recovery rather than interfere with it. In practice, that means the peel itself remains a medical procedure, while the surrounding skincare can be selected with equal attention to tolerability, sourcing, and regulatory compliance.
Why Swiss clients ask different questions
Swiss clients are often well read, but their understanding is usually consumer-level rather than procedural. They may know terms like “acid,” “frosting,” or “downtime,” yet still misread what they will see in the mirror over the following days.
The same misunderstandings appear often in clinic:
- More visible peeling means a better result: Clinical success depends on appropriate depth, even application, and correct aftercare. Heavy flaking alone is not a quality marker.
- Natural aftercare means weaker aftercare: Barrier-supportive formulas can be both well formulated and aligned with a cleaner ingredient philosophy, provided they avoid common irritants and unsupported claims.
- A professional peel and an at-home peel are close substitutes: They differ in concentration, skin preparation, endpoint assessment, risk control, and legal responsibility.
That last point deserves emphasis. A supervised TCA peel is more than “stronger skincare.” It is a controlled injury performed with intent, training, and clear rules around who should be treated, how the skin is prepared, and how recovery is monitored.
Why this treatment keeps gaining ground
TCA matches the expectations of a patient group that wants visible change without an overly complicated plan. Many patients are less interested in collecting products than in following a structured protocol that makes sense from consultation to re-epithelialisation.
That has changed how clinicians need to communicate. Good candidates are rarely reassured by vague promises. They respond better when you explain the treatment in concrete terms: what the peel is meant to correct, what day-by-day recovery tends to look like, why the mouth or chin may peel more than the cheeks, and which post-procedure products are chosen because they support healing rather than because they fit a marketing trend.
From a practice perspective, this is why TCA continues to hold its place in Swiss aesthetics. It fits a medical model that values precision, and it can also fit a modern clean-beauty framework, as long as the clinician keeps the hierarchy clear. The acid does the corrective work. Aftercare protects the repair process. Ethics in sourcing are welcome, but they never replace clinical judgment.
How TCA Peeling Renews the Skin
TCA renews skin by creating a precise chemical injury in the outer layers, then relying on the skin’s own repair machinery to rebuild a smoother, more even surface. For new clinicians, the key is to stop thinking only about “peeling” and start thinking about protein coagulation, inflammation, re-epithelialisation, and remodelling.
In practice, the visible flaking is only one chapter of the story.

What TCA is doing in the skin
Trichloroacetic acid is a keratocoagulant. It denatures proteins in treated tissue. That action disrupts parts of the epidermis that are rough, photo-damaged, or unevenly pigmented, and it sets off a wound-healing response that replaces them with better organised tissue.
A practical way to teach this is to separate what the eye sees from what the biology is doing. The eye sees whitening, tightness, darkening, and peeling. The biology is handling controlled coagulation first, then inflammation, then repair.
The sequence usually looks like this:
Application
TCA is applied in a consistent pattern to skin that has been degreased and assessed zone by zone.Protein coagulation
The acid interacts with epidermal proteins. This creates the visible endpoint called frosting.Inflammatory signalling
Cytokines and other repair signals are released, beginning the healing cascade.Shedding of altered tissue
The treated surface becomes dry, taut, and often darker before it starts to detach.Re-epithelialisation and remodelling
New epidermal cells cover the surface. Over time, dermal repair can improve texture, pigment irregularity, and fine lines.
For clinicians working in a Swiss setting, this distinction matters because patients increasingly ask for treatments that feel compatible with a cleaner, lower-toxicity lifestyle. The physiology does not change. TCA remains the active corrective step. Ethically sourced and well-formulated aftercare can support barrier recovery, reduce irritation from unnecessary additives, and align with patient values, but it does not replace the chemistry of the peel itself.
What frosting means
Frosting is one of the most misunderstood parts of a TCA peel. It is the visible effect of protein coagulation, not a measure of bravery, and not a sign that more layers are automatically better.
A useful analogy for trainees is heat on egg white. As proteins denature, the appearance changes. Skin proteins respond differently, of course, but the visual principle helps people understand why the surface turns pale or white.
The clinical question is not whether frosting appears. The clinical question is what pattern appears, how quickly it develops, and whether it matches the intended depth for that anatomical site.
A good peel is usually quiet in the treatment room. Even coverage, careful observation, and restraint produce better outcomes than dramatic endpoints.
Why peeling can look uneven
Patients often expect one neat sheet of skin to lift away. Real skin behaves more like a patchwork, because different facial zones have different thickness, sebaceous activity, sun history, and mechanical stress.
That is why recovery often looks uneven:
- Around the mouth peeling may appear earlier because speaking, eating, and facial expression create constant movement
- Cheeks often show broader flaking because they are relatively dry and commonly carry more cumulative UV injury
- The T-zone may peel less dramatically on the surface, even when the peel has still had a clinical effect
- Periocular skin responds differently because it is thinner and requires greater caution in product choice and technique
Swiss climate adds another variable. Cold air, wind, indoor heating, and altitude can increase transepidermal water loss during recovery. A patient in Geneva in winter may describe more tightness than the same patient would after a similar protocol in a milder season. That does not mean the peel has gone deeper. It often means the barrier is losing water faster and needs disciplined post-procedure support.
Visible peeling isn’t the whole result
The result you are aiming for is not a dramatic shed. It is better skin quality after healing.
Some patients desquamate in visible sheets. Others show only fine scaling. Both patterns can be compatible with improvement if the indication was correct, the endpoint was well judged, and the recovery phase was managed properly.
This point is especially useful when speaking to patients drawn to natural beauty messaging. They may focus on what they can see and feel each day, and they may assume that “more peeling” means “more detox” or “more renewal.” It is better to explain that the skin is repairing itself according to depth, site, and individual biology. The clinician’s role is to guide that repair with evidence-based care, including bland barrier-supportive formulations and, where appropriate, carefully selected products with simple plant-derived ingredients that are low in fragrance and irritation risk.
Document texture, pigment pattern, oiliness, and healing day by day. That record is more reliable than the patient’s memory of how much skin came off.
A Guide to TCA Concentrations Depths and Timelines
Peel depth determines which skin layer you are treating, how much visible peeling a patient may see, and how long recovery usually lasts. A superficial TCA peel stays within the epidermis. A medium-depth peel reaches into the papillary dermis. That distinction matters more than the bottle percentage alone.
For new clinicians, this is often the first point of confusion. Patients ask for a “strong peel,” but the correct question is narrower: what depth is needed for this complaint, on this skin, in this season, under this level of supervision? In Swiss practice, where dry winter air, altitude, and strict safety expectations all influence recovery planning, that framing leads to better decisions.
The practical way to think about depth
TCA concentration gives you a starting estimate, not a guaranteed endpoint. Depth is shaped by several variables acting together: skin preparation, the number of passes or layers, pressure, anatomical site, barrier condition, and the patient’s own healing response.
That is why two patients treated with the same percentage can peel very differently.
A useful clinical habit is to map the problem before choosing the peel. Broad dullness and mild roughness usually call for a lighter approach. Established acne scarring or more fixed textural change may justify a medium-depth plan if the patient is suitable. Tools such as a skin analyser machine can support this assessment by documenting pigment distribution, oil pattern, pore visibility, and surface irregularity before treatment. The device does not replace judgement, but it can sharpen it.
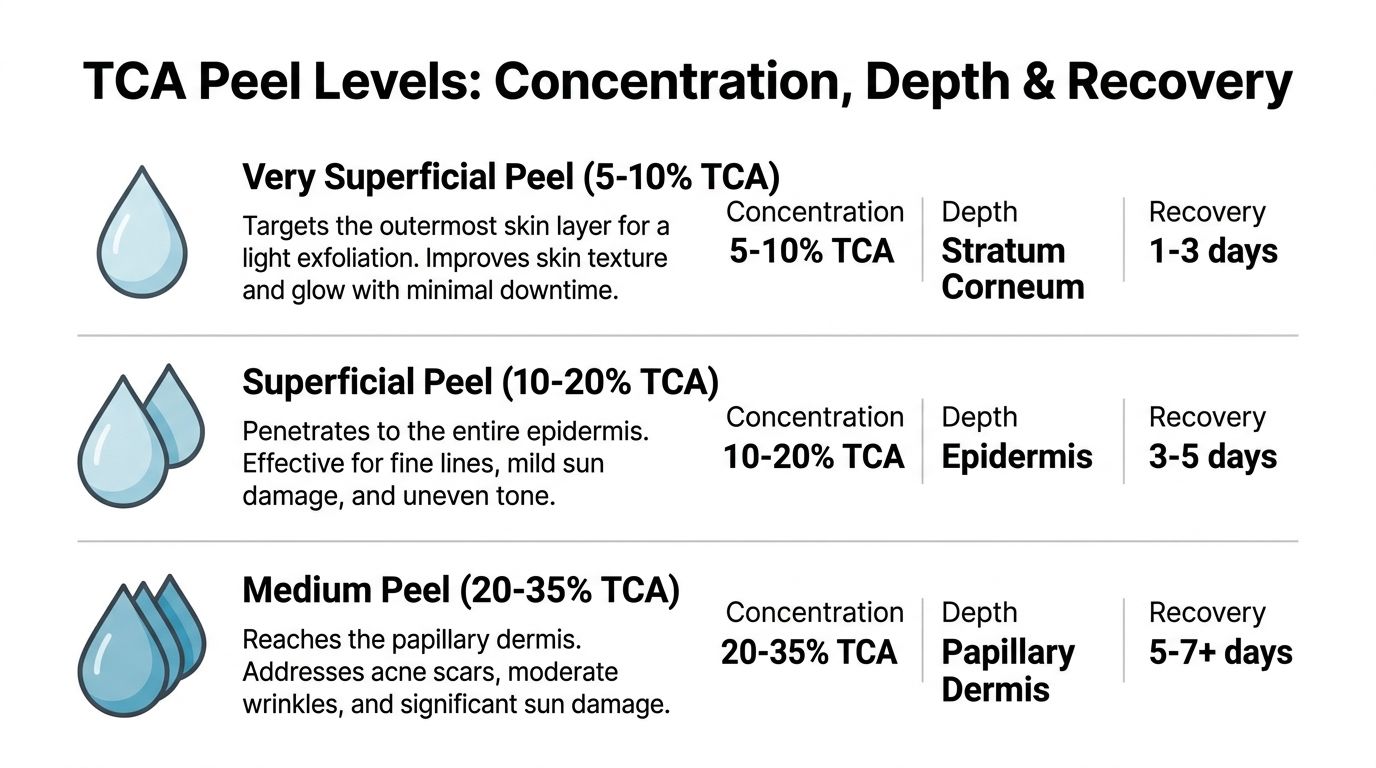
TCA Peel Depth Comparison
| Peel Depth | TCA Concentration | Target Skin Layer | Expected Peeling & Downtime | Primary Indications |
|---|---|---|---|---|
| Very superficial | 5-10% | Stratum corneum | Light dryness or fine flaking, short recovery | Dullness, mild roughness, tone refresh |
| Superficial | 10-20% | Epidermis | Noticeable flaking, tightness, visible shedding over several days | Fine lines, mild uneven tone, mild photodamage |
| Medium | 20-35% | Papillary dermis | More obvious peeling, stronger tightness, longer recovery | Acne scarring, more established pigment, textural change |
These are teaching ranges. Real-world outcomes depend on technique and patient selection. Clinical reviews of chemical peeling describe TCA as a depth-dependent procedure in which concentration, application method, and skin characteristics all affect penetration and healing pattern, as outlined in this peer-reviewed review of chemical peels in aesthetic practice.
What the patient usually notices first
Patients do not feel “15%” or “25%.” They notice sequence.
With a lighter peel, the usual story is tightness first, then fine flaking, then a quicker return to a socially comfortable appearance. With a medium-depth peel, the sequence is often more distinct. Early stinging or heat is followed by tightening, a darker or bronzed look, then more visible peeling, and finally a pinker, more delicate surface.
That sequence is useful in consultation because it replaces vague language with something observable.
Why concentration is only one part of the plan
New clinicians sometimes treat percentage as if it were the whole prescription. It is only one dial on the control panel.
Visible response can change with:
- Skin thickness
- Sebum output
- Recent retinoid use or over-exfoliation
- Barrier stability
- Treatment area
- Application uniformity
- Pre-peel conditioning
- Climate and season
Swiss conditions matter here. A patient treated in a heated alpine environment may report more tightness and dryness than a patient treated under milder conditions, even when the peel depth is similar. Recovery advice should reflect that reality, especially if your clinic also serves patients who prefer minimalist or plant-based skincare. “Natural” aftercare still needs to be low-irritant, fragrance-controlled, and barrier-focused.
How to match depth to the complaint
Match the depth to the pathology, not to the patient’s appetite for dramatic peeling.
For diffuse dullness or very mild textural change, a very superficial or superficial approach is often enough. For dyschromia, photodamage, or acne scarring, the treatment plan may need greater depth or a staged series. The safer rule is to start with the lightest peel that can realistically address the indication, then reassess after healing.
This is the clinical bridge between medical peeling and the clean beauty movement. Patients may ask for “natural renewal” and fear anything that sounds aggressive. You can address that concern directly. The acid itself is a controlled medical tool. The surrounding protocol, including ethically sourced cleansers, bland barrier creams, and carefully screened botanical ingredients, can still align with a cleaner formulation philosophy without lowering safety standards.
Timelines patients can understand
Use plain timelines. They improve consent and reduce anxious follow-up messages.
Very superficial
The skin may feel dry or slightly rough for a short period, with fine flaking or almost no visible shedding.
Superficial
Tightness usually appears first. Flaking often becomes noticeable over the next several days.
Medium
Redness and tightening are usually followed by darkening, more obvious peeling, and then a pink new surface that needs disciplined photoprotection and gentle care.
Do not promise an identical day-by-day course for every patient. Give a range and explain what can shift it.
Where clinicians get into trouble
Complications often begin with poor interpretation, not poor chemistry.
A clinician may mistake minimal visible peeling for treatment failure. Another may equate heavier shedding with a better result. A patient may tolerate discomfort well, but tolerance does not make the endpoint safer. These errors are common because TCA gives strong visible cues, and visible cues are easy to overvalue.
Precision matters more. Choose the endpoint carefully, document the baseline clearly, and teach patients that better skin quality after healing is the goal. Visible peeling is only one part of that process.
Identifying Ideal Candidates and Contraindications
A good TCA peel starts before the first drop touches the skin. Candidate selection is where outcomes are protected.
Some patients are suitable because the indication is clear and the risk profile is manageable. Others may be technically interested but clinically unsuitable at that moment. New clinicians must learn to say, “not yet”, or sometimes, “not for you”.
The patient profile that fits best
TCA is often a strong option for patients with visible textural change, photoageing, post-acne marks, or selected pigment concerns. In Swiss studies, combination TCA-lactic acid peels showed 82% efficacy in acne scar reduction and 65% melasma clearance after 4-6 treatments, while the wider Swiss peel market generates over CHF 120 million, with 40% involving TCA, according to this Swiss clinical and market review of chemical peels.
That tells you two things. First, this isn’t a fringe treatment. Second, the indication still matters more than popularity.
What I want to know before I approve treatment
During consultation, I want answers to these areas before I decide on depth or timing:
- Pigment behaviour: Does the patient form post-inflammatory hyperpigmentation easily?
- Inflammation history: Have they had eczema flares, rosacea instability, or recurrent facial irritation?
- Healing tendency: Any history of abnormal scarring?
- Current routine: Are they using retinoids, exfoliating acids, scrubs, or irritating actives?
- Lifestyle exposure: Will they respect strict UV avoidance and aftercare?
A visual device can help standardise this stage. In practices that want more structured baseline imaging and surface assessment, a skin analyser machine can support documentation and patient education before a peel plan is finalised.
Contraindications that should stop or delay treatment
Some situations call for postponement. Others rule the treatment out unless a medical plan changes first.
Absolute or strong stop signs
- Active infection: Herpetic lesions, bacterial infection, or uncontrolled inflammatory eruptions
- Compromised skin barrier: Raw, abraded, or recently overtreated skin
- Unreliable aftercare adherence: A patient who won’t follow instructions is not a good peel candidate
- Unrealistic expectations: If they expect one peel to erase every lesion, stop and reframe
Relative caution areas
- Darker or reactive skin types: These patients may still be treated, but require conservative planning and pigment-risk counselling
- Rosacea-prone skin: Not impossible, but not casual
- Recent irritation from home actives: Delay until the skin is stable
- History of aggressive DIY peels: Investigate what was used and how the skin responded
The consultation isn’t paperwork. It’s the first safety intervention.
The question behind the question
When a patient asks, “Am I a good candidate?”, they’re usually asking something deeper.
They mean one of three things:
- Will this work for my problem?
- Will I peel in a way I can tolerate socially?
- Will I end up worse than I started?
Your answer should address all three. That’s how you reduce anxiety and improve consent quality.
Mastering Pre and Post Peel Care with Natural Formulations
A common Swiss clinic scenario goes like this. The peel itself is performed correctly, the endpoint is appropriate, and the patient still returns worried on day four because the skin feels tight, the flakes look uneven, and the products at home are stinging. In most cases, the problem is not the TCA. The problem is the care around it.
That is why pre and post peel planning deserves the same discipline as the procedure. Swiss patients move between heated indoor air, cold dry weather, and strong reflected UV with very little warning. A recovery plan that ignores those conditions is incomplete.

Natural formulations can fit well into peel care, but only if they behave like good medical aftercare. The goal is low irritancy, barrier support, and patient adherence. Ethical sourcing and clean labels may matter to Swiss patients, especially in wellness-led practices, yet those values should sit on top of physiology, not replace it.
Before the peel
Pre-peel care is preparation of the barrier. A well-prepared barrier is like priming a wall before paint. If the surface is already inflamed, dry, or patchy, the result is less predictable.
I teach clinicians to focus on three practical tasks.
- Reduce unnecessary actives: Stop the products that keep the skin in a low-grade irritated state.
- Support the barrier: Use bland hydration and a gentle, non-foaming cleanser.
- Set social expectations: Explain clearly when redness, tightness, and visible shedding are most likely.
A natural-leaning routine can work here if it stays restrained. Sulphate-free cleansing, fragrance-light moisturisers, and carefully chosen lipid-rich products may support tolerance. “Botanical” is not automatically gentle. Many plant extracts and essential oils are far more reactive than patients realise.
Day-by-day recovery that clinicians can teach
Patients do better with a timeline they can picture. After a TCA peel, the skin usually follows a sequence. First inflammation, then drying and visible separation, then fragile renewal. If you explain the sequence in advance, fewer patients misread normal peeling as a complication.
Day 1 to Day 2
This is the tight, warm, sunburn-like stage.
The skin may look pink or red and feel taut. Some clients worry because nothing is peeling yet. Reassure them that visible shedding often starts later.
Priorities:
- Cleanse gently: Use lukewarm or cool water and a non-foaming cleanser.
- Protect the surface: Apply a plain reparative balm in a thin, even layer.
- Avoid friction: No scrubs, brushes, washcloths, or rubbing.
- No actives: Retinoids, exfoliating acids, and strong vitamin formulas should stay out.
For clean-beauty aligned practices, a well-made marine or barrier balm can be appropriate at this stage. It should function like clinical aftercare. Texture, tolerability, and ingredient restraint matter more than marketing language.
Day 3 to Day 5
This is when tca peel peeling usually becomes visible.
The skin often darkens first, then begins to crack, flake, or lift. Around the mouth and nose, peeling may start earlier. The cheeks may lift in broader sheets, while the T-zone can look less dramatic. Patients often assume uneven peeling means uneven treatment. More often, it reflects differences in oil production, movement, and local barrier thickness.
This is also the stage where patients create avoidable injury.
- Don’t pick
- Don’t roll the skin off
- Don’t exfoliate the flakes away
- Don’t try to speed the process up
If the skin feels very tight, an occlusive, ECOCERT-aligned balm may reduce friction and limit additional irritation. This is an effective way to bridge clinical peeling with a natural product philosophy. Choose the product because it suits healing skin and fits your formulation standards, not because it sounds wholesome.
To help clients visualise the day-by-day peeling stages and understand what not to do, this short video provides a clear, patient-friendly overview:
Day 6 to Day 7 and beyond
By this point, much of the visible peeling may be settling. The skin often looks smoother and brighter, but it is still immature. New epidermis behaves like fresh varnish on wood. It may look dry before it is ready for more product, and it marks easily if exposed to irritation or UV. Overconfidence often causes trouble at this stage. Patients often restart retinoids, acids, scrubs, or active serums too early because the peeling has stopped. Stopping visible flaking is not the same as full barrier recovery.
How to combine natural formulations without becoming careless
Natural aftercare should be boring in the best possible sense. After a peel, the skin does not need stimulation. It needs a quiet environment to rebuild.
Use natural formulations for support, not stimulation
Good choices usually include:
- Soap-free cleansers
- Barrier-focused balms
- Simple hydrating creams
- Selected organic oils only if the barrier is not actively irritated
Poor choices include products sold as “renewing”, “active”, “tingling”, or “detoxifying”. Those cues often signal fragrance, exfoliants, acids, or essential oils, all of which can disturb healing skin.
Match the product to the stage
A clinician should prescribe by phase, not by brand story.
| Recovery stage | Skin state | Best product type |
|---|---|---|
| Early recovery | Warm, tight, vulnerable | Bland cleanser, protective balm |
| Active peeling | Dry, cracking, flaky | Occlusive barrier support, minimal routine |
| Post-peel pinkness | Delicate, reactive | Calm hydration, strict UV protection |
That framework also helps with product selection in Swiss practices that want ethically sourced or naturally derived lines. If a formula cannot meet the needs of the stage, its sourcing credentials do not rescue it.
Address Swiss climate directly
Swiss aftercare needs local realism. Indoor heating dries the air. Winter air can leave the skin feeling tighter and more brittle. High altitude and reflected light increase UV exposure even on cool or cloudy days. Patients often underestimate that risk because the skin does not feel hot.
Translate that into specific instructions:
- Winter recovery: prioritise occlusion and remind patients to avoid over-cleansing in dry indoor environments
- Summer recovery: increase UV avoidance discipline, not just sunscreen use
- High-altitude routines: hats, shade, and timing matter as much as the product itself
A patient who spends the weekend in Verbier after a peel has different recovery demands from a patient staying indoors in Geneva. Aftercare should reflect that.
Products and ingredients to keep out
Every clinic needs a simple exclusion list during healing.
Avoid:
- Exfoliating acids
- Retinoids
- Strong essential oil blends
- Physical scrubs
- Highly fragranced creams
- Anything that stings on application
If a product creates heat, sting, or visible flushing, it has no role in routine recovery care. Simple products are often the safest and, for this phase, the most appropriate choice.
The Swiss Regulatory Environment and Mitigating Risks
A patient books a peel in Zurich on Friday, then spends Sunday skiing above the tree line. The treatment itself may be well executed, yet significant risk can come from something less dramatic: a clinic that has not matched the procedure, the setting, and the follow-up plan to Swiss rules and Swiss conditions.
That is the starting point for compliance in Switzerland. For chemical peels, you should not rely on US agencies or generic beauty-industry summaries. Swiss practices need to work from Swiss law and Swiss authorities, particularly the Federal Act on Medicinal Products and Medical Devices, the Federal Act on Protection against Dangerous Substances and Preparations, and guidance from Swissmedic and the Federal Office of Public Health. If a clinic cannot identify the legal basis for who may perform a peel, under what supervision, and with what documentation, the protocol is incomplete.

In practice, the question is simple. Is this being handled as a low-risk cosmetic service, or as a procedure that requires medical assessment, medical responsibility, or both? TCA is not regulated by marketing language. A bottle described as professional, clean, botanical, or natural does not change the duty to assess risk correctly.
What compliance means in practice
Compliance starts before the first pass of acid. It works like a chain of custody in pharmacy practice. If one link is weak, the whole system is less safe.
A Swiss clinic protocol should define:
- Who assesses the patient: not only who applies the peel, but who decides that the patient is an appropriate candidate
- Which product is being used: full ingredient list, concentration, intended use, supplier documentation, and traceability
- What level of supervision applies: based on the formulation, the treatment goal, the patient’s risk profile, and cantonal practice requirements
- How consent is documented: indication, expected downtime, pigment risk, and when to seek urgent review
- Who manages complications: with a named clinician and a clear contact pathway
That last point matters. Complications rarely announce themselves during office hours.
The main risks to control
Pigment change
Post-inflammatory hyperpigmentation is a clinical risk, not a marketing problem. It is more likely when depth selection is poor, inflammation runs longer than expected, or UV exposure is underestimated. In Switzerland, mountain exposure and reflected light add a layer of risk that urban patients often miss.
The practical lesson is straightforward. A technically correct peel still needs a prevention plan for pigment. That includes conservative patient selection, disciplined endpoint recognition, and aftercare that supports barrier recovery without unnecessary irritants.
Overtreatment
Newer clinicians often focus on the peel solution and forget the skin in front of them. TCA behaves differently on sebaceous forehead skin, thin periocular skin, and skin already stressed by winter dryness, retinoids, or unreported home exfoliation.
A good operator reads tissue response the way a pilot reads weather. You do not argue with the conditions. You adjust the plan or you postpone.
Safer practice usually looks quieter than aggressive marketing suggests:
- fewer passes when the endpoint appears early
- different treatment intensity by facial zone
- deferral when the barrier is unstable or the history is unclear
- lower tolerance for improvisation in patients with pigment tendency
Product and sourcing confusion
The clean beauty movement has raised useful questions about sourcing, preservatives, fragrances, and environmental burden. Those questions belong in Swiss aesthetic medicine. They do not replace toxicology, sterility, or documentation.
For that reason, ethically sourced aftercare can fit well into a peel protocol, but only if the product can do the clinical job. A balm derived from alpine botanicals may be attractive to a Swiss patient. The clinician still has to ask the harder questions. Is the formula low-irritant? Is fragrance absent or minimal? Is batch quality consistent? Can the supplier provide documentation that would stand up to professional scrutiny?
Natural positioning is therefore a filter, not a licence.
A Swiss standard worth aiming for
The strongest model for Swiss practice is integrated care. The procedure follows medical discipline. The recovery plan can include well-chosen, ethically sourced formulations that respect both skin physiology and patient values. That approach fits the Swiss market because patients often expect both. They want evidence, and they want ingredient integrity.
Used properly, regulation supports that model. It separates careful clinical work from casual peel culture, and it protects the patient, the clinician, and the reputation of the practice.
Answering Your Client's Top TCA Peel Questions
The best consultation answers are calm, direct, and specific. Patients don’t need a lecture. They need an explanation they can hold onto when they’re standing in front of a mirror on day four.
Why didn’t I peel as much as my friend
Because your skin isn’t your friend’s skin.
Peeling varies with skin thickness, oiliness, facial movement, prior sun damage, and barrier condition. Around the mouth, peeling is often earlier and more obvious. On an oilier T-zone, it may be much less visible. A lighter visible peel doesn’t automatically mean a poor treatment.
Tell the patient this: the aim was controlled renewal, not a competition in flaking.
Is it safe to have a TCA peel during the Swiss summer
It can be, but only in a carefully selected patient who will follow strict UV avoidance.
Summer in Switzerland isn’t harmless just because the air feels cooler than in southern climates. Mountain exposure, reflected light, and outdoor habits all matter. If a patient has a hiking holiday, lake weekend, or prolonged sun exposure planned, reschedule. The best peel timing is the one that allows disciplined recovery.
What’s the difference between a TCA peel and a laser treatment
A helpful way to phrase it is this: both can resurface, but they do it through different forms of controlled injury.
TCA is a chemical injury. Laser is device-based energy. One isn’t automatically superior. The better option depends on pigment tendency, texture goals, downtime tolerance, skin history, and what the clinic can deliver safely.
Patients often assume lasers are more advanced because they are more expensive or more technical-looking. That’s not a reliable guide. The correct treatment is the one matched properly to the problem.
My skin feels extremely tight and itchy. Is that normal
Often, yes. Tightness and itch can be part of normal healing, especially as the old surface dries and begins to lift.
What you want to know is whether the symptom is expected or excessive. Mild to moderate tightness, dryness, and itch can occur during active peeling. Worsening pain, spreading inflammation, abnormal discharge, or a healing pattern that looks wrong should trigger clinical review.
A useful script for patients is simple:
- tight is common
- itchy can happen
- picking is not allowed
- worsening pain is not normal
Why is one side of my face peeling more than the other
Human faces are not symmetrical in behaviour.
Patients sleep on one side, drive with one side more exposed to light, touch one side more often, and carry different barrier stress across the face. Application pattern also matters. Mild asymmetry in visible peeling can happen without indicating a failed treatment.
The key question is whether the skin is healing evenly enough, not whether every flake appears at the same hour.
Can I use my favourite “natural” serum while I’m peeling
Usually not if it’s active, fragranced, acidic, or stimulating.
Patients often hear “natural” and think “safe during recovery”. That’s a mistake. During the peel window, the right products are the least exciting ones. Gentle cleanser, protective balm, simple hydration, and UV discipline. Their favourite serum can come back later, once the barrier has recovered and you say it’s appropriate.
Your consultation should make recovery feel predictable. Patients cope well when they know what is normal, what is not, and what they must leave alone.
When should I worry
Give patients a short escalation rule they can remember.
Contact the clinic if they notice:
- increasing rather than settling pain
- unusual crusting or discharge
- a healing pattern that suddenly worsens
- concerning darkening after the peel that doesn’t fit the expected course
That short list reassures good patients and identifies real problems earlier.
If you’re building a Swiss peel offering that combines clinical credibility with ethically sourced aftercare, beautysecrets.agency can help you source premium natural and professional skincare lines suited to pharmacies, spas, wellness centres, and aesthetic practices that want a stronger clean-beauty proposition.


